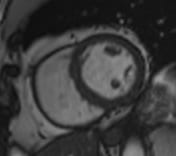
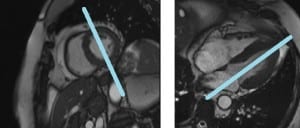
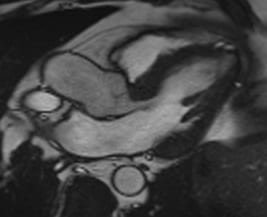
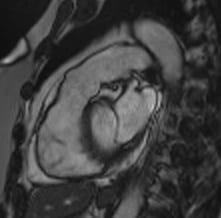
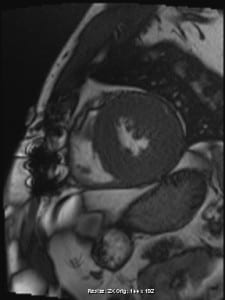
Short Axis
The short axis view will provide us information about the walls of the heart.
This is plotted as a slab from the apex of the heart through the tricuspid and mitral valves.
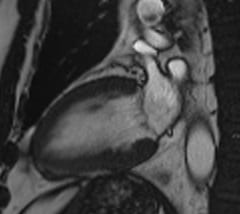
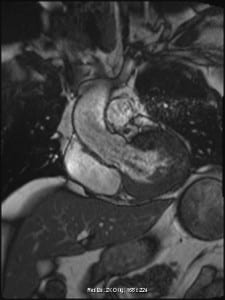
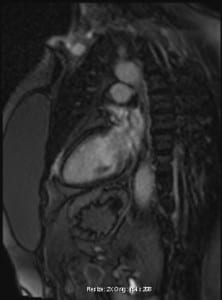
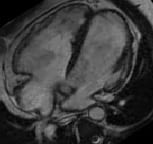
Left 2 Chamber
The 2 chamber view demonstrates the left side of the heart in profile. The mitral valve will be seen.
This is usually plotted as one slice.
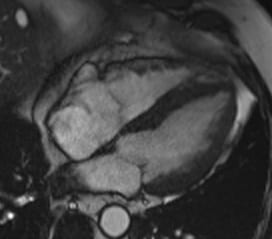
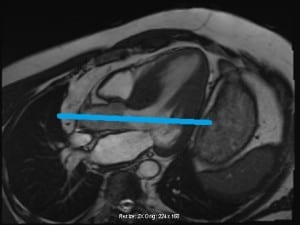
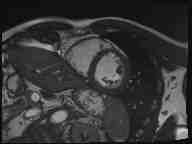
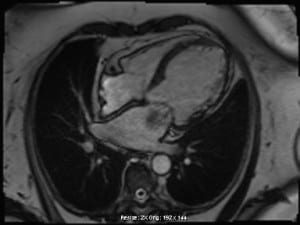
4 Chamber
The 4 chamber view provides us a picture of the heart where both ventricles and atria are seen as well as the tricuspid and mitral valves.
This is usually plotted as one slice.
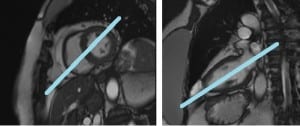
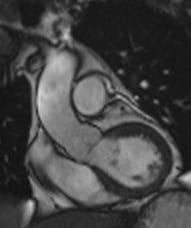
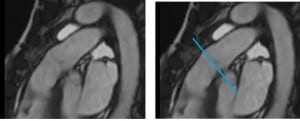
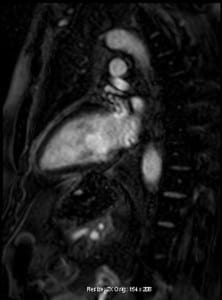
3 Chamber
This view allows us to visualize blood entering and leaving the left ventricle. We can visualize blood entering through the mitral valve and leaving through the aortic valve.
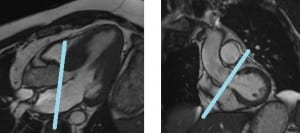
This has one slice plotted through the LVOT on the short axis view.
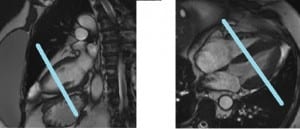
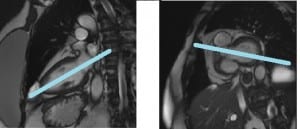
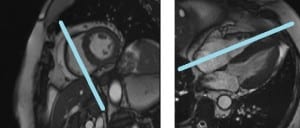
LVOT
The left ventricular outflow tract evaluates blood and corresponding structures as it leaves the heart.
Here, we need to plot perpedicular to the aortic valve on the 3 chamber view and parallel to the LVOT.
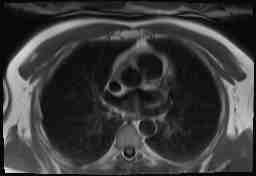
RVOT
The right ventricular outflow tract evaluates blood flowing out of the right ventricle and entering the pulmonary artery.
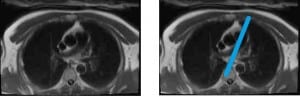
For this view, the recommendation is to select an orthagonal transaxial image and find the pulmonary artery. Following this, we need to plot parallel to the pulmonary artery.

RT 2 Chamber
This view will place the right ventricle and atrium in profile. We can then evaluate the tricuspid valve.
This slice will bisect the tricuspid valve on the 4 chamber view and be parallel to the septum on the short axis view.

Pulmonic Valve
During CMR on a pulmonic valve slice, we can evaluate the opening and closing of the pulmonic valve and/or measure velocities of blood flowing through.
Here, the recommendation is to plot parallel to the pulmonic valve on the RVOT view

Aortic Valve
During CMR on an aortic valve slice, we can evaluate the opening and closing of the aortic valve and/or measure velocities of blood flowing through.
Here, we plot parallel to the aortic valve on the 3 chamber and LVOT view.
Pulse Sequences
Listed below are some of the most common MR parameters and/or pulse sequences used to evaluate the heart and its associated cardiovascular structures
Single Shot Fast Spin Echo
SS-FSE is routinely used to perform dark blood sequences and evaluate pertinent anatomical structures. There are many benefits to performing SS-FSE in cardiac imaging . For instance, such sequences are useful for correcting/remedying arrhythmia and other motion-related artifacts. They are also less sensitive to inhomogeneous fields which is helpful for susceptibility- artifact-correction-techniques
Gradient Echo
These sequences are typically spoiled gradients (incoherent gradient echoes) – and – therefore promote T1 weighting in our image. Compared to other gradient echoes, they may be less susceptible to inhomogeneous fields. Such sequences – are – thus – prone to susceptibility artifacts from implanted devices. Additionally, Gradient Echo Cardiac MR sequences are known to demonstrate bright blood in resultant images.

Steady-State Free Precession
These sequences involve promoting a unique T2/T1 image contrast. Additionally, SS-FP sequences offer us faster scan times, better CNR, and improved SNR – imaging options. These sequences are known to demonstrate bright blood in our image. On that note – For CINE imaging – the recommendation is to choose either the gradient echo or steady-state echo – sequences
Flow Imaging
When evaluating flow, the recommendation is to used a Phase Contrast (PC) technique. This will allow us to measure the velocity of blood moving through our patient. We must select the appropriate velocity encoding (VENC) value when performing such flow sequences
CINE
This technique involves monitoring cardiovascular structures during rhythmic cardiac function. The images are obtained with ECG-triggered segmented imaging. It is, therefore, very useful for evaluating cardiac activity.
T1/T2 Mapping
This technique is useful for getting a more in-depth understanding of myocardium tissue. It will require obtaining hematocrit labs prior to imaging. MyoMap sequences can be performed to acquire either T1 or T2 / pre-contrast or post- contrast images.

Inversion Recovery
These sequences are typically performed post contrast and utilized as late enhancement techniques. On that note; a Phase – Sensitive Inversion recovery (PSIR) sequence, demonstrates applicable sensitivity for infarct.
Infarct
Infarcts happen to be some of the most common anomalies seen on a cardiac MR exam. CINE sequences demonstrating sensitivity to irregular myocardial wall function and late Gadolinium- enhanced sequences evaluating the endocardium for damaged tissues are – significant – for diagnosing/analyzing infarcts. When an infarct extends into the myocardium – we refer to this – as transmural infarct. The extent of the infarct into the myocardium will determine the viability of affected tissue.
![]()
The location and/or extent of gadolinium enhancement can identify the affected/ involved cardiac vessels
Cardiomyopathy
Cardiomyopathy chronicles the associated diseases of and/ or relating to the cardiac muscles. Many variations of cardiomyopathy have been identified in scientific/medical literature today. These anomalies are best identified through and/or are particularly sensitive to Functional Imaging. Late gadolinium enhancement is also great at evaluating any resultant scarring.
Dilated Cardiomyopathy
This is demonstrated as “thinning of the myocardium”

Hypertrophic Cardiomyopathy
This particular anomaly signals the “thickening of the myocardium”
Restrictive Cardiomyopathy
In this instance of Cardiomyopathy, the heart experiences difficulties during contractions and becomes too rigid to expand. The heart is unable to pump properly as it becomes harder for the associated ventricles to obtain enough blood. This, in turn, obstructs the relaxation mechanism relevant to cardiovascular function.
Arrhythmogenic Right Ventricular Dysplasia (ARVD)
This type of Cardiomyopathy is known to be extremely rare. It can be identified by the fat deposits in the myocardium.
Mass
Cardiac/Cardiovascular structures can be susceptible to masses/abnormal growths/tumors. Such anomalies can range from benign cysts to metastatic/malignant tumors. Depending on the location of said mass, the consulting radiologist may order a particular/preferred Cardiac MR views/views. Dynamic Imaging is particularly useful for the evaluation of such pathologies

Valve Disease
Cardiac Valves are susceptible to anomalies due to issues within/pertaining to flow mechanism:
1) Regurgitation: This involves blood flowing backwards through a valve. The particular defect can be seen on the side of a valve where the blood just came from/originated.
2) Turbulent flow: This involves a jet of and/or high velocity flow in the direction of flowing blood. This occurs when valves are not opening properly.